Thoraco-abdominal aortic aneurysm: symptoms appear when the condition is already serious. How to treat microinvasively and surgically at Monza Ares
There are diseases that give no signs when the condition becomes serious. The thoracic-abdominal aortic aneurysm is one of them. Discovering early and treated in specialized centers, however, it offers real chances of complete recovery – including through microinvasive solutions available in Romania.
Aortal aneurysm represents an abnormal dilation of the main artery of the body – aorta – which can evolve for years without symptoms. When this dilation affects both the thoracic and the abdominal segment, we are talking about thoracic-abdominal aneurysm-one of the most complex forms of this pathology.
Symptoms are missing or easily ignored
One of the biggest challenges in the case of thoracic-abdominal aneurysm is that it does not hurt, does not warn and, most of the times, does not offer any clear clues, in the early and intermediate phases. The disease evolves in silence, sometimes years in a row, and the symptoms – when they appear – are often non -specific or confused with other conditions.
Persistent abdominal or lumbar pain, pressure sensation, breathing difficulties caused by compression on neighboring organs – all may occur late, when aneurysm has increased significantly or is close to rupture.
In many cases, the condition is discovered by chance, following a recommended imaging investigation for a completely different reason. Unfortunately, if aneurysm is diagnosed in a critical stage, the risk of rupture is extremely high, and the mortality rate can reach up to 90%.
The causes of aneurysm differ depending on the location, but are commonly encountered in smoking people – including those who have quit smoking – and elderly patients, with untreated high blood pressure or hypercholesterolemia. People who have relatives in the family diagnosed with aortic aneurysm have a higher probability of developing the same condition. It is more common in men over 65 years, but it can also occur in younger people, if there are genetic predispositions or vascular trauma.
“The treatment depends on several factors: the size of the aneurysm, the growth rate and the anatomy of the patient. If the size is below 5 cm and stable, periodic monitoring is recommended through imaging investigations. Over 5.5 cm or in case of rapid evolution, the intervention becomes essential. At Monza Ares, the treatment is personalized. Each case is analyzed within a case Heart Team – a multidisciplinary medical team consisting of specialists in clinical cardiology, interventional cardiology, cardiovascular surgery, vascular surgery, imaging and intensive therapy. This integrated approach allows to establish the best therapeutic behavior and reduce the associated risks. ” confirms Dr. Călin Popa, head of the Vascular Surgery Section at Monza Bucharest Hospital.
Combined Evar and Tevar intervention, made microinvasively, in a single procedure
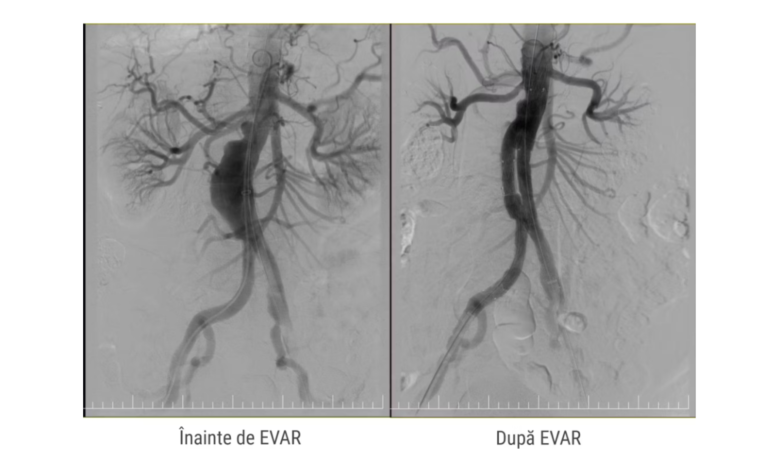
When anatomy allows, medical teams choose the Evar/Tevar procedure-(thoracic) endovascular aneurysm Repair-a micro-invasive intervention, through which the aneurysms of the chest (tevar), abdominal (EVAR) are treated or, in some cases, both at the same time, through a single combined procedure. The actual intervention involves the introduction through the femoral artery in the groin area of a thin catheter with special stent-a metal tube covered with synthetic material-which is guided to the level of aneurysm. Once reached the right place, the stent opens and seals the fragile aortic wall, redirecting the blood flow through its interior, which reduces the risk of rupture.
“It all starts from an extremely precise planning. The patient is image assessed by angio-art, to see exactly the shape, size and location of the aneurysm. Based on these data, a stent-graph adapted to its anatomy, explains Dr. Stefan Moț, primary doctor of interventional cardiology.

The benefits for the patient are clear: in tevar and evar procedures, access to the vascular system is commonly achieved by arterial puncture, compared to classic surgical incisions, 5-7 cm, which means minimal trauma, reducing the risk of complications and faster postoperative recovery. In some cases, the medical team can opt for a combined intervention, in which Tevar and Evar are performed in a single microinvasive procedure, which allows the simultaneous treatment of the thoracic and abdominal segments of the aorta, thus reducing the need for several separate interventions.
In certain situations – such as small diameter femoral arteries, severe calcifications or anatomical abnormalities – the medical team can opt for a limited surgical incision, for several centimeters, to facilitate access to the artery. Even in these cases, the intervention remains much less invasive than classical surgery, being part of what we call endovascular approach.
Most of the time, the procedure is performed without general anesthesia, and in most cases, with reduced postoperative pain and discharge, usually in 2-3 days. Post-evar monitoring is essential, to verify the stability of the stent and the complete exclusion of the aneurysm from the circulation.
“The cases of thoracic-abdominal aneurysm are among the most difficult treatment, but also the most spectacular from the perspective of the results obtained with micro-invasive solutions.
“From the preoperative planning based on a high precision angio-art, to the millimeter positioning of the stent, every detail is vital. Therefore, the approach in an integrated center such as Monza Ares makes the difference,” adds Dr. Dan Deleanu, primary interventional cardiology doctor.
When surgery is the only option
A recent case treated at Monza Ares shows how important the quick and coordinated intervention is. A 71 -year -old patient, with multiple comorbidities and a history of aortic interventions, was urgently admitted. The investigations highlighted a bulky aneurysm that had come to affect the left lung. The intervention, conducted by the team led by Dr. Călin Popa, a primary cardiovascular surgery, lasted about 6 hours and involved the affected segment of the aorta and its reconstruction. The patient recovered completely, without complications.
In very complex cases, where the patient's anatomy does not only allow endovascular approach, hybrid interventions can be resorted – which combines open surgery with endovascular techniques. Monza Ares, the largest cardiology network and the most experienced private operator in microinvasive cardiology in Romania, has the necessary infrastructure – hybrid room, level I and a vast experience – to safely intervene even in the most difficult cases.
“We have the ability to intervene surgery in complete safety, with access to the necessary resources and a team prepared for the most difficult cases,” says Dr. Călin Popa.
About the Monza Ares group
The Monza Ares group is the largest private national network specialized in cardiology, offering therapeutic solutions of microinvasive cardiology through cardiovascular surgery and interventional cardiology. Monza Ares owns Category I, 5 operating rooms dedicated to cardiovascular surgery and 3 angiography rooms within the Monza Hospital, in total with 11 angiography rooms in 8 centers in Bucharest, Cluj-Napoca, Constanța, Târgu Jiu, Tulcea, Onești and 3 multidisciplinary clinics, with Focus on Cardiology- Cardiomed. The Monza Ares mission in Romania is to ensure the access of as many patients as possible to innovative treatments in the sphere of cardiology. In the spirit of this mission, during the 15 years of activity, 22 national medical premieres took place in Monza Ares. Since 2019, the group has been mostly owned by the American Highlander Partners investment fund.
Article supported by Monza Ares





